Rev Med UAS
Vol. 10: No. 4. Octubre-Diciembre 2020
ISSN 2007-8013
Jesús Gilberto Arámburo-Gálvez1, MSc; María de los Ángeles Sabaté2, BSc; Ingrid Wagner2, BSc; Gimena Valeria Alfonsina Dezar2, MSc; Marcela de Jesús Vergara-Jiménez3,PhD; Noé Ontiveros4,PhD; Francisco Cabrera-Chávez3,PhD; Feliznando Isidro Cárdenas-Torressup3*,PhD.
*Corresponding Author: Feliznando Isidro Cárdenas-Torres.
Avenida Cedros y Calle Sauces S/N Fraccionamiento Los Fresnos, Culiacán, Sinaloa, 80246, México.
Email address: feliznando@uas.edu.mx
DOI http://dx.doi.org/10.28960/revmeduas.2007-8013.v10.n4.006
Recibido 30 de Agosto 2020, aceptado 10 de Septiembre 2020
RESUMEN
Objetivos: La información sobre la epidemiología de las alergias alimentarias (AA) en Latinoamérica es escasa permaneciendo incierta la magnitud y relevancia del problema. Nuestro objetivo fue estimar la prevalencia de AA en niños de edad escolar de Santa Fe, Argentina. --- Material y Métodos: Padres de niños de 5-14 años de edad contestaron un cuestionario validado el cual fue auto-administrado. Resultados: 1431 cuestionarios fueron regresados con respuestas válidas. Las prevalencias fueron [intervalos de confianza (IC), 95%]: “Reacciones adversas a los alimentos” 10.2% (8.7-11.9), “AA percibida, transitoria” 9.7% (8.3-11.4), “diagnóstico médico de AA, transitoria” 4.8% (3.8-6), “AA tipo inmediato, transitoria” 3.4% (2.6-4.5), “AA tipo inmediato, persistente” 1.4% (0.9-2.1), “anafilaxis inducida por alimentos” 0.8% (0.5-1.5). Los principales alimentos desencadenadores de “AA tipo inmediato, persistente” fueron: chocolate y chile (0.49% cada uno, IC 95%: 0.24-1.01), seguido de cacahuate, nueces y trigo (0.14% cada uno, IC 95%: 0.04-0.51). Tener antecedentes familiares de enfermedades alérgicas se relacionó positivamente con “AA tipo inmediato, transitoria” (P = 0.0002). Aunque ocho de 12 casos de anafilaxis buscaron atención médica, solo uno de estos casos reportó la prescripción de un auto-inyector de epinefrina. --- Conclusiones: Al menos 1.4% de los niños argentinos experimentan reacciones adversas a los alimentos sugestivas de AA de tipo inmediato y al menos la mitad de ellos necesitan una prueba confirmatoria y asesoramiento por un profesional de la salud. Debido a la baja frecuencia de prescripción de auto-inyectores de epinefrina en casos de anafilaxis, su uso debe alentarse entre los profesionales de la salud.
Palabras clave: Alergia alimentaria; Prevalencia; encuesta.
ABSTRACT
Objectives: There is scarce information about the epidemiology of food allergy (FA) in the Latin America region and remains uncertain the magnitude and relevance of the problem. Our aim was to estimate the prevalence of FA in schoolchildren from Santa Fe, Argentina. --- Material and Methods: A validated self-administered Spanish version of a structured questionnaire was utilized. Parents of 5-14-years-old children participated in the study. Results: 1,431 questionnaires were returned with valid responses (response rate of 35.3%). Prevalence estimations (CI, 95%) were as follows: “Adverse food reactions” 10.2% (8.7-11.9), “Perceived FA, ever” 9.7% (8.3-11.4), “Physician-diagnosed FA, ever” 4.8% (3.8-6), “Immediate-type FA, ever” 3.4% (2.6-4.5), “Immediate-type FA, current” 1.4% (0.9-2.1), “Food-induced anaphylaxis” 0.8% (0.5-1.5). The main foods triggering “Immediate-type FA, current” were: chocolate and chili (0.49% each, CI 95%: 0.24-1.01), followed by peanut, nuts and wheat (0.14% each, CI 95%: 0.04-0.51). Family history of allergic disease was positively related to ‘immediate-type FA, ever’ (P = 0.0002). Although eight out of 12 cases of anaphylaxis sought medical attention, only one of these cases reported the prescription of an epinephrine auto-injector. --- Conclusions: The data highlight that at least 1.4% of Argentinian schoolchildren experience adverse food reactions suggestive of immediate-type FA and that at least half of these cases need confirmatory testing and counseling by a health professional. Due to the low frequency of prescription of epinephrine auto-injectors in anaphylactic cases, the prescription of such devices should be encouraged among healthcare personnel.
Keywords: Food allergy, Prevalence, Survey.
Introduction
Food allergy (FA) is a persistent and potentially severe condition that negatively impacts on the quality of life of both allergic children and adults. The prevalence of this immunological disorder is thought to be increasing and could affect 2-4% and 6-8% of the adult and child populations, respectively.1 Annually, more than 30,000 North Americans seek medical attention due to moderate or severe food allergic reactions. Unfortunately, around 50% of the severe anaphylactic cases die.1 The prevalence of FA in children is well documented in developed countrie,2 but it is not in developing regions. For instance, only three population-based studies have used an in depth instrument to estimate the parent-reported prevalence of FA in Latin American schoolchildren.3-5 Particularly, the Latin American region encompasses a big area with different sociocultural practices and socioeconomic factors, which influence the alimentary habits in children6 and probably the prevalence rates of FA and the specific foods triggering it as well. Therefore, much remains to be explored in Latin America in order to know the magnitude and relevance of the FA problem. Thus, the aim of this study was to estimate at population level the parent-reported prevalence of FA in schoolchildren from Santa Fe, Argentina.
Material and Methods
Population survey
A population-based cross-sectional study was conducted in Santa Fe, Argentina from April 3rd to 20th 2018. Six public and 3 private elementary schools geographically distributed at the northwest, center, and south of the city were chosen by convenience. At least two schools per area and 15 children per grade were included in the study (at least 105 children per school). The teachers (1st to 7th grade) handed out the questionnaires and the informed consents. All documents were attached to the children’s homework notebooks. In the cases of non-response by the parents, the process was repeated for additional two times.
Questionnaire and Definitions
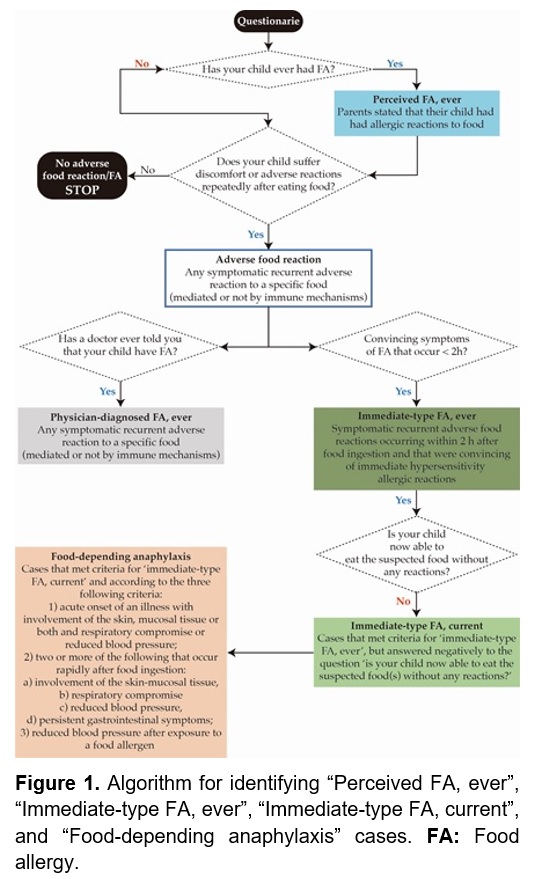
A Spanish version of a structured questionnaire (3) was culturally adapted (minor changes) and self-administrated by Argentinian parents (supplemental material). The definitions used in this study are shown in Figure 1 (4,5).
Statistical analyses and ethical aspects
Descriptive statistics and two-tailed Fisher exact tests were carried out using PASW statistic software version 25.0 (SPSS Inc., IL, USA). Continuous variables were summarized by mean and the minimum and maximum values. A P-value < 0.05 was considered statistically significant. OpenEpi software (3.03a) was used to estimate prevalence confidence intervals (CI, 95%). An Ethics Review Board of the Faculty of Biochemistry and Biological Sciences of the National University of the Litoral approved the study protocol (ethic approval number: Acta 01/18).
Results
Demographic and clinical information
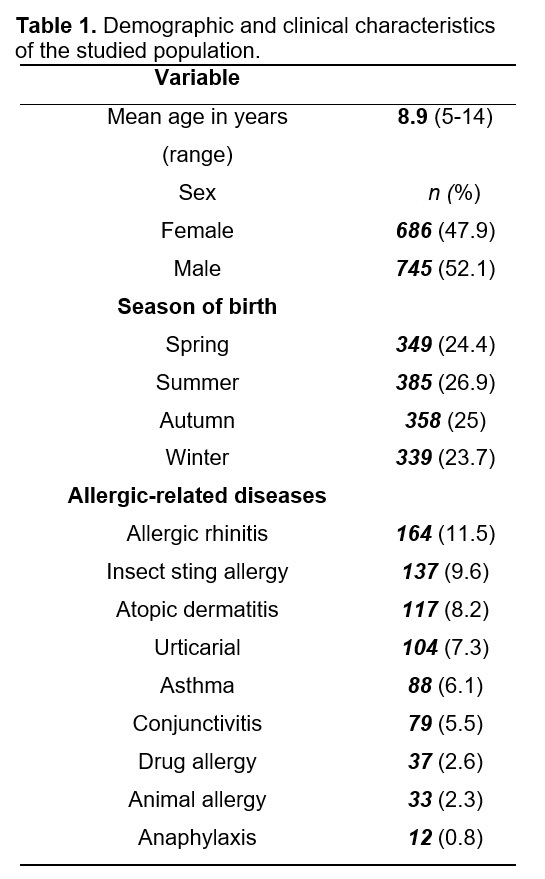
The demographic and clinical characteristics of the participants are shown in Table 1. The response rate was 35.3% [1,431 questionnaires were correctly answered (738/693 public/private schools)]. The proportion of female/male was 47.9%/52.1% (P > 0.9999). A family history of allergic disease (first degree relatives) and having an allergic disease other than FA were parameters associated with “Immediate-type FA, ever” (P < 0.001).
Prevalence estimations of adverse food reactions and FA
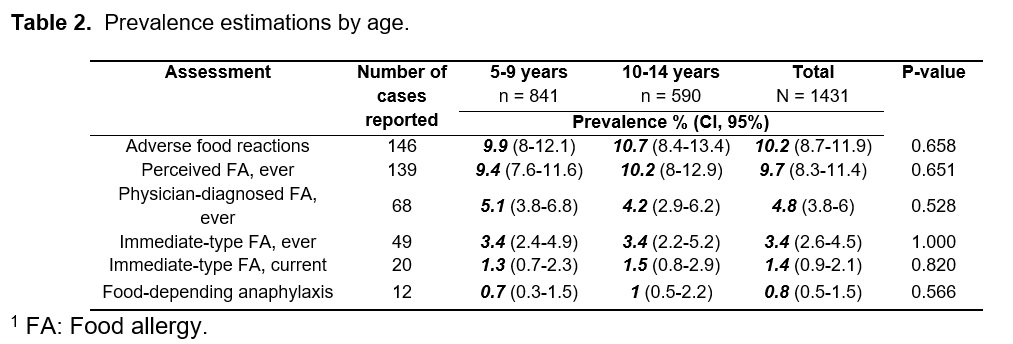
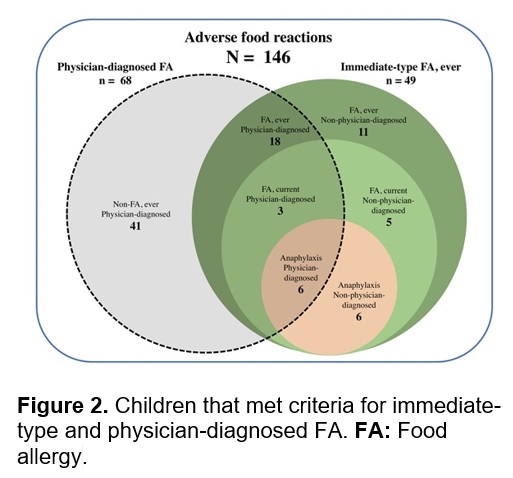
The prevalence estimations by age groups are summarized in Table 2. Twenty-seven cases that met criteria for immediate-type FA, either “ever” or “current”, reported a physician-diagnosed FA (Figure 2). Stratified by gender, the prevalence rates of immediate-type FA, either “ever” or “current”, were quite similar (P > 0.9999 in both cases). Eight out of 12 cases of anaphylaxis sought medical attention. Corticoids, an inhalator, and an epinephrine auto-injector were prescribed in one case each. The season of birth was not associated with “immediate-type FA” (P > 0.6552).
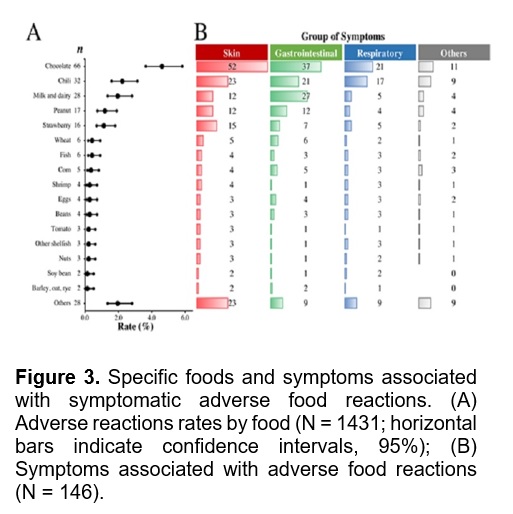
Foods causing symptomatic adverse reactions in schoolchildren
The most common foods causing adverse reactions and the specific symptoms associated with them are shown in Figures 3A and 3B, respectively. Ninety-eight cases (67.1%) sought medical attention and 41 (28.1%) reported adherence to a restrictive diet (2 cases had no “physician-diagnosed FA, ever”).
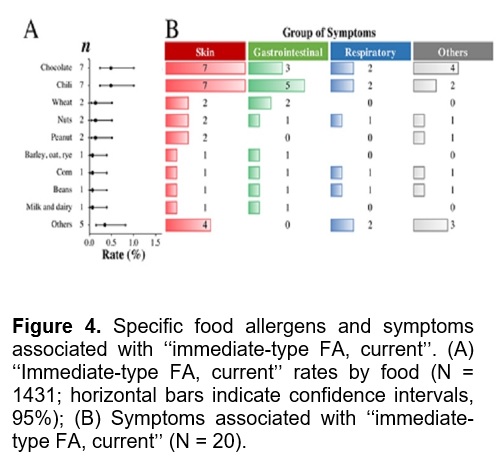
Common food allergens and clinical characteristics of FA
The most common foods causing “immediate-type FA, current” and the symptoms associated with them are shown in Figures 4A and 4B, respectively. Together, chocolate and chili accounted for 48.3% of the “immediate-type FA, current” cases and triggered 66.6% of the cases of anaphylaxis (n = 8). Other foods that triggered anaphylaxis were wheat (n = 2), milk and dairy, peanuts/chocolate, nuts, (n = 1 each).
Discussion
The present study shows that adverse food reactions are common in Argentinian schoolchildren and that 1.4% of the children meet criteria for “Immediate-type FA, current”. This is the lowest FA prevalence rate reported in Latin American schoolchildren. Studies carried out in Chile, Mexico, and El Salvador reported FA prevalence rates from 3.5% to 5.5% using the same definitions of FA.3 Other survey studies carried out in Latin America reported FA prevalence rates from 14.9% to 23.5%, but the target population and the definitions of FA were different.7 The prevalence rates of chocolate and chili allergy in Argentinian schoolchildren (0.5%) were similar to those reported in Chile (0.8%)3 and Mexico (0.5%)4 and this is in line with the notion that the consumption of chili8 and chocolate9 is widespread in western countries. However, none of the Argentinian schoolchildren met criteria for shrimp or shellfish allergy, which were the most common food allergens reported in Mexican schoolchildren.4 Similarly, shrimp and shellfish were food allergens frequently reported in Chilean and Salvadoran schoolchildren.3-5. Argentinian parents did not report cases of egg allergy although this food is a known allergen that affects children from the Latin American region and other regions from North America, Asia, and Europe.2,4,10 Due to sociocultural practices and socioeconomic factors widely differ among Latin American countries and these aspects influence the children’s alimentary habits,6 main food allergens are expected to differ among different Latin American regions.
The prevalence rate of anaphylaxis in Argentinian schoolchildren was 0.8%. This prevalence rate is lower than the rates reported in Chilean (2.6%), Mexican (1.2%) and Salvadoran (2.5%) schoolchildren, which were estimated using the same definitions of anaphylaxis.3-5 Notably, only 1 out of 12 Argentinian schoolchildren that met criteria for food-induced anaphylaxis was advised to acquire an epinephrine autoinjector despite this device is the preferred emergency treatment for anaphylactic cases. Previous studies documented the lack of prescription of epinephrine autoinjectors in Argentina11 and in other Latin American countries.3-5 Notably, different from other countries in the Latin American region, epinephrine autoinjectors are commercially available in Argentina and this can help to increase awareness about the use and prescription of the autoinjectors by patients and healthcare personnel, respectively.
The main strengths of this study are its population-based design and the use of a validated in depth instrument previously utilized in other Latin American countries, which allows fair comparisons of the results. Furthermore, it has been described that the use of in depth instruments provides a fairly high detection efficiency (56-93%) (12,13). We should acknowledge that our study has some limitations. Firstly, the relatively low response rate (35.3%) could impact on the prevalence estimations. It is expected that individuals with knowledge about the disease studied would be more prompted to take the survey, however, this notion seems not to be the rule in the present study since the estimated prevalence rate of “immediate-type FA, current” is the lowest reported ever in Latin American schoolchildren. And secondly, our results were not corroborated with laboratory tests or other allergy tests commonly carried out in clinical practice, e.g. skin prick tests evaluations with fresh food extracts. Despite these limitations, our study provides useful epidemiological data regarding FA in Argentinian schoolchildren and serves as the groundwork for further epidemiological studies based on objective diagnostic criteria.
Conclusion
This is the first population-based study conducted in Argentina to estimate the prevalence of FA. The parent-reported prevalence of FA in Argentinian schoolchildren was 1.4% and it is the lowest prevalence rate reported until now among Latin American countries. Due to the prescription of epinephrine auto-injectors in cases that met criteria for food-induced anaphylaxis is uncommon, the prescription and use of this emergency device should be encourage among health care professionals and anaphylactic individuals, respectively.
Acknowledgements
We acknowledge the postgraduate fellowships given to F.I.C.-T and J.G.A.-G by the Mexican Council for Science and Technology (CONACyT).
Referencias